Eye Anotomy:
Function of the Eye:
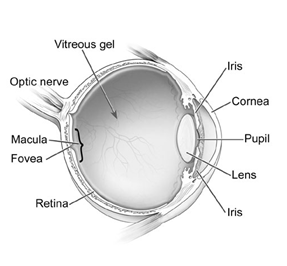
The eye has many parts that work together to provide the clear vision we view our environment with. Often referred to as a camera, the eye converts light into electrical signals, which when transformed in the brain, give us the images we see of the world.
Structures of the Eye
Cornea: The first area that light enters the eye. It is kept moist with constant tear production. Dry eyes can affect the image that passes through this structure, making it blurry.
Pupil: The size of the pupil determines how much light can enter the eye. When it is constricted (small) it allows less light in, and when it is dilated (large), it lets more light in. When your pupil is dilated, it allows for a more thorough internal eye exam.
Iris: This the coloured portion of your eye, and it is responsible for changing the diameter (size) of the pupil in response to the light in your environment.
Lens: This structure focuses the light on your retina, and changes in shape when reading things up close or observing something out in the distance. As we age, it looses its flexibility, limiting the ability to adjust to these changes. This results in the need for reading glasses later in life.
Vitreous: This is the jelly substance that fills the interior of the eye. It is here that is responsible for the production of floaters, small shadows cast in your vision.
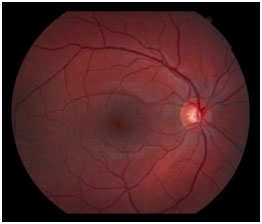
Retina: This thin tissue layer acts like the film in the camera, capturing the light and transforming it into the electrical signals for the brain. It is has many blood vessels to nourish it like other organs of the body, and it has areas responsible for fine detail, colour vision, and peripheral vision.
Macula/Fovea: The macula is used for colour vision and the fine details we are able to see. The fovea is at the centre of the macula, where the concentration of the cells needed for central vision is the highest. It is here where diseases such as AMD are so damaging, resulting in a loss of this central vision.
Optic Nerve: the transmission system from the retina, to your brain to produce the images you see in front of you.
-
What is age-related macular degeneration?
Age-related macular degeneration (AMD) is a disease that blurs the sharp, central vision you need for “straight-ahead” activities such as reading, and driving. AMD affects the macula, the part of the eye that allows you to see fine detail. AMD causes no pain. It does not affect your peripheral vision. In some cases, AMD advances so slowly that people notice little change in their vision. In others, the disease progresses faster and may lead to a loss of vision in both eyes. AMD is a leading cause of vision loss in patients 60 years of age and older. As the name describes AMD is a degeneration of the macula. The macula is the name given to the center of the retina, the light-sensitive tissue at the back of the eye. The retina converts light into electrical impulses. The retina then sends these impulses, or nerve signals, to the brain.

-
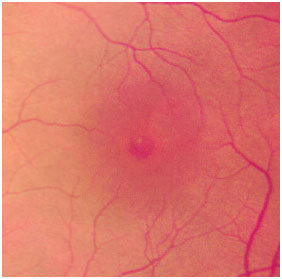
What are dry and wet AMD?
Dry AMD occurs when the light-sensitive cells in the macula slowly break down, gradually blurring central vision in the affected eye. As dry AMD gets worse, you may see a blurred spot in the center of your vision. Over time, as less of the macula functions, central vision in the affected eye can be lost gradually. The most common symptom of dry AMD is slightly blurred vision. Dry AMD generally affects both eyes, but vision can be lost in one eye while the other eye seems unaffected. Wet AMD occurs when abnormal blood vessels behind the retina start to grow under the macula. These new blood vessels tend to be very fragile and often leak blood and fluid. The blood and fluid raise the macula from its normal place at the back of the eye. Damage to the macula, and therefore to vision occurs rapidly. With wet AMD, loss of central vision can occur quickly. Wet AMD is considered to be advanced AMD and is more severe than the dry form. An early symptom of wet AMD is that straight lines appear wavy. If you have vision loss from dry or wet AMD in one eye only, you may not notice any changes in your overall vision. With one eye seeing clearly, you still can drive, read, and see fine details. You may notice changes in your vision only if AMD affects both eyes. Dry AMD is much more common than wet. More than 85 percent of all people with AMD have the dry form. However in those with significant vision loss from AMD about two-thirds of patients have the wet form. All people who have the wet form had the dry form first. The dry form can advance and cause vision loss without turning into the wet form. The dry form also can suddenly turn into the wet form, even during early stage AMD. There is no way to tell if or when the dry form will turn into the wet form.
-
Who is at risk for AMD?The main risk factors for AMD are age and family history (genetics). Women appear to be at greater risk than men. The only modifiable risk factors are smoking, obesity and high blood pressure so these should be addressed to decrease your risk of vision loss. An Amsler grid should be used to watch for a change in vision that may suggest wet AMD is developing. The pattern of the grid resembles a checkerboard. You will cover one eye and stare at a black dot in the center of the grid at 12 inches distance. While staring at the dot, you may notice that the straight lines in the pattern appear wavy. Sudden changes in the grid appearance should be reported to our office.
-
What treatment can be considered for AMD?
The National Eye Institute’s Age-Related Eye Disease Study (AREDS) found that taking a specific high-dose formulation of antioxidants and zinc significantly reduces the risk of advanced AMD and its associated vision loss. Slowing AMD’s progression from the intermediate stage to the advanced stage will save the vision of many people. The specific daily amounts of antioxidants and zinc used by the study researchers were: 500 mg of vitamin C, 400 IU vitamin E, 15 mg beta-carotene (often labeled as equivalent to 25,000 IU of vitamin A), 80 mg of zinc as zinc oxide, and 2 mg of copper as cupric oxide. Copper was added to the AREDS formulation containing zinc to prevent copper deficiency anemia, a condition associated with high levels of zinc intake. Smokers need to take a modified version of the supplement without added beta-carotene due to an increased risk of lung cancer. (Vitalux-S is one available formulation) More recent evidence suggests that Omega-3 from fish oils or flax seed oils is also beneficial at reducing the risk of progress in macular degeneration. Caretoids such as Lutein and Zeaxanthine are also felt to have a protective effect and may be beneficial. The AREDS vitamins, Omega-3 and caretoids are not a cure for AMD. They will not restore vision already lost from the disease. However, they may delay the onset of advanced AMD. It may help people who are at high risk for developing advanced AMD to keep their vision. The high levels of vitamins and minerals are difficult to achieve from diet alone. However, previous studies have suggested that people who have diets rich in green leafy vegetables have a lower risk of developing AMD. In addition the levels of antioxidants and zinc are considerably higher than the amounts in any daily multivitamin. A multivitamin contains many important vitamins not found in the AREDS formulation. You may want to take a multivitamin along with the AREDS formulation. For example, people with osteoporosis need to be particularly concerned about taking vitamin D, which is not in the AREDS formulation.
Wet AMD is treated with eye injections Lucentis or Avastin. These are special medicines which cause the abnormal blood vessels under the retina to shrink, but not permanently disappear. This allows the fluid within and under the retina to go away. These injections have been shown to be very effective in preventing further vision loss (90% of eyes) and often allow vision to improve (35% of eyes). Unfortunately, these injections are treatments rather than a cure for AMD and you will require multiple injections on an on-going basis. Your treatments for AMD may also include laser surgery including photodynamic therapy. The disease and loss of vision may progress despite treatment. The type and possibility for treatment depends on characteristics of the wet AMD and will be discussed with you by your doctor. Your lifestyle can play a role in reducing your risk of developing AMD. Eat a healthy diet high in green leafy vegetables and fish. Also don’t smoke, maintain normal blood pressure, maintain a healthy body weight and exercise regularly.
-
What happens during the eye injections?
Anesthetic drops will be applied to freeze the surface of your eye. A speculum (spring) will be used to hold your eye open. An iodine solution will then be placed on the surface of the eye to sterilize it. You will be asked to look up or behind you to correctly rotate your eye. The medicine will then be injected by your specialist. It is normal to feel a sharp pinch, pressure or popping sensation at the time of the injection. Any discomfort is usually temporary. The remaining iodine solution will then be flushed from your eye. It is normal for the eye to be red after the procedure. New temporary floaters are also common.
-
What is a cataract?
A cataract is a change of the lens in the eye that affects vision. The lens is a clear part of the eye that helps to focus light, or an image, on the retina. The retina is the light-sensitive tissue at the back of the eye. It acts like the film in a camera.
In a normal eye, light passes through the transparent lens to the retina. Once it reaches the retina, light is changed into nerve signals that are sent to the brain.
The lens must be clear for the retina to receive a sharp image. If the lens is cloudy from a cataract, the image you see will be blurred.
Most cataracts are related to aging. Cataracts are very common in older people. By age 80, more than half of our population either have a cataract or have had cataract surgery.
A cataract can occur in either or both eyes. It cannot spread from one eye to the other.
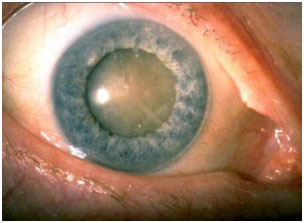
A cataract is a haziness that develops within the lens of the eye. Symptoms include glare, haziness of vision or decreased vision. Cataract do not damage the eye, but they can reduce the ability of a patient to do the things they would like such as driving or reading fine print. If a cataract is bad enough to affect function, then surgery can be performed to remove the hazy lens and replace it with a clear artificial lens.
-
How do cataracts develop?Age-related cataracts develop in two ways:
Clumps of protein reduce the sharpness of the image reaching the retina. The lens consists mostly of water and protein. When the protein clumps up, it clouds the lens and reduces the light that reaches the retina. The clouding may become severe enough to cause blurred vision. When a cataract is small, the cloudiness affects only a small part of the lens. You may not notice any changes in your vision. Cataracts tend to “grow” slowly, so vision gets worse gradually. Over time, the cloudy area in the lens may get larger, and the cataract may increase in size. Seeing may become more difficult. Your vision may get duller or blurrier.
The clear lens slowly changes to a yellowish/brownish color, adding a brownish tint to vision. As the clear lens slowly colors with age, your vision gradually may acquire a brownish shade. At first, the amount of tinting may be small and may not cause a vision problem. Over time, increased tinting may make it more difficult to read and perform other routine activities.
-
Who is at risk for cataract?
The risk of cataract increases as you get older. Other risk factors for cataract include certain diseases (for example, diabetes), personal behavior (smoking, alcohol use), environment (prolonged exposure to ultraviolet sunlight). As well it is very common to develop cataract following other intraocular surgery – ie. Retina surgery for various eye disease.
-
What are the symptoms of a cataract?
- Cloudy or blurry vision
- Colors seem faded
- Glare: Headlights, lamps, or sunlight may appear too bright. A halo may appear around lights
- Poor night vision
- Double vision or multiple images in one eye. (This symptom may clear as the cataract gets larger)
- Frequent prescription changes in your eyeglasses or contact lenses.
These symptoms also can be a sign of other eye problems. If you have any of these symptoms, check with your eye care professional.
-
How is a cataract treated?
The symptoms of early cataract may be improved with new eyeglasses, brighter lighting, anti-glare sunglasses, or magnifying lenses. If these measures do not help, surgery is the only effective treatment. Surgery involves removing the cloudy lens and replacing it with an artificial intraocular lens (IOL).
A cataract needs to be removed only when vision loss interferes with your everyday activities, such as driving, reading, or watching TV. You and your eye care professional can make this decision together. Once you understand the benefits and risks of surgery, you can make an informed decision about whether cataract surgery is right for you. In most cases, delaying cataract surgery will not cause long-term damage to your eye or make the surgery more difficult. You do not have to rush into surgery.
Sometimes a cataract should be removed even if it does not cause problems with your vision. For example, a cataract should be removed if it prevents examination or treatment of another eye problem, such as age-related macular degeneration or diabetic retinopathy.
-
What are the risks of cataract surgery?As with any surgery, cataract surgery poses risks, such as infection and bleeding. Cataract surgery slightly increases your risk of retinal detachment. Other eye disorders, such as high myopia (nearsightedness), can further increase your risk of retinal detachment after cataract surgery. You need to discuss the risks with your cataract surgeon.
-
Can problems develop after surgery?
Problems after surgery are rare, but they can occur. These problems can include infection, bleeding, inflammation (pain, redness, swelling), loss of vision, double vision, and high or low eye pressure. With prompt medical attention, these problems usually can be treated successfully.
Sometimes the eye tissue that encloses the IOL becomes cloudy and may blur your vision. This condition is called an after-cataract. An after-cataract can develop months or years after cataract surgery. An after-cataract is treated with a laser. Your doctor uses a laser to make a tiny hole in the eye tissue behind the lens to let light pass through. This outpatient procedure is called a YAG laser capsulotomy. It is painless and rarely results in increased eye pressure or other eye problems. As a precaution, your doctor may give you eyedrops to lower your eye pressure before or after the procedure.
-
When will my vision be normal again?
You can return quickly to many everyday activities, but your vision may be blurry. The healing eye needs time to adjust so that it can focus properly with the other eye, especially if the other eye has a cataract. Ask your doctor when you can resume driving.
If you received an IOL, you may notice that colors are very bright. The IOL is clear, unlike your natural lens that may have had a yellowish/brownish tint. Within a few months after receiving an IOL, you will become used to improved color vision. Also, when your eye heals, you may need new glasses or contact lenses.
-
Diabetic Retinopathy
Diabetic retinopathy is damage that can occur at the back of the eye from diabetes. Diabetic retinopathy can include bleeding, leaking, formation of new blood vessels, or retinal detachment. Regular examinations and treatment when necessary can reduce the risk of vision loss dramatically. Good blood sugars and good blood pressures also reduce the risk of developing diabetic retinopathy by greater than 50%.Diabetic retinopathy is a complication of diabetes and a leading cause of blindness. It occurs when diabetes damages the tiny blood vessels inside the retina, the light-sensitive tissue at the back of the eye. A healthy retina is necessary for good vision. If you have diabetic retinopathy, at first you may notice no changes to your vision. But over time, diabetic retinopathy can get worse and cause vision loss. Diabetic retinopathy usually affects both eyes.
-
What are the stages of diabetic retinopathy?
Mild Nonproliferative Retinopathy
At this earliest stage, microaneurysms occur. They are small areas of balloon-like swelling in the retina’s tiny blood vessels. Moderate
Nonproliferative Retinopathy
As the disease progresses, some blood vessels that nourish the retina are blocked.
Severe Nonproliferative Retinopathy
Many more blood vessels are blocked, depriving several areas of the retina with their blood supply. These areas of the retina can produce chemical signals which can stimulate the growth of new abnormal retinal blood vessels.
Proliferative Retinopathy
At this advanced stage, the growth or proliferation of new abnormal blood vessels has occurred. This condition is called proliferative retinopathy. These new blood vessels are abnormal and fragile. They grow along the retina and along the surface of the clear, vitreous gel that fills the inside of the eye. By themselves, these blood vessels do not cause symptoms or vision loss. However, they have thin, fragile walls. If they leak blood, severe vision loss and even blindness can result.
-
Who is at risk for diabetic retinopathy?
All people with diabetes–both type 1 and type 2–are at risk. That’s why everyone with diabetes should get a comprehensive dilated eye exam at least once a year early in diabetes and more frequently as directed by their ophthalmologist. Approximately 25% of Canadians diagnosed with diabetes have some stage of diabetic retinopathy. If you have diabetic retinopathy, we may recommend treatment to help prevent worsening of your eye disease.
-
How does diabetic retinopathy cause vision loss?
Fluid can leak into the center of the macula, the part of the eye where detailed central vision occurs. The fluid makes the macula swell, blurring vision. This condition is called macular edema. It can occur at any stage of diabetic retinopathy, although it is more likely to occur as the disease progresses. About half of the people with proliferative retinopathy also have macular edema.
Fragile, abnormal blood vessels can develop and leak blood into the vitreous chamber in the center of the eye, blurring vision. This is called a vitreous hemorrhage. The abnormal blood vessels (neovascularization) that grow with proliferative retinopathy can contract and pull on the retina. In some cases this contraction can cause retinal detachment.
-
Does diabetic retinopathy have any symptoms?
Diabetic retinopathy often has no early warning signs. Don’t wait for symptoms. Make sure to keep your appointments and see your retina specialist as directed. However, possible symptoms can range from mild blurring of vision to sudden near complete visual loss.
-
How diabetic retinopathy treated?
In recent years there have been new advances in the treatment of diabetic retinopathy:
1) Focal retinal laser: Significant macular edema can often be treated with laser. The small leaky blood vessels are targeted and treated so they no longer leak. The procedure is not painful, although the laser light can be bright. It takes only a few minutes to do the procedure although it takes a few months for the eye to stop leaking. Often more than one treatment is needed to stop the leakage. New areas of leakage can develop or treated areas may start leaking again so continued follow up with your retina specialist is necessary. Focal laser treatment helps to preserve vision. In fact, focal laser treatment has been shown to reduce the risk of vision loss by 50 percent. It can also improve the vision in some people.
2) Pan retinal laser photocoagulation (PRP): This is an important treatment for proliferative diabetic retinopathy. The oxygen and nutrient starved peripheral retina produces the chemical signals that causes the abnormal blood vessels to grow. Ablation of the peripheral retina is performed with laser to shut down the production of this chemical signal. This allows the abnormal blood vessels to shrink away. More laser spots with more power are required for this treatment compared to focal laser. As a result, this procedure can sometimes be painful. Because a high number of laser spots are necessary, three or more sessions usually are required to complete treatment. Side effects of PRP can include loss of your side vision, color vision or night vision. However, it is an essential treatment to protect vision.
3) Injections: More recent research and experience has lead to the use of eye injections for the treatment of diabetic retinopathy. Both Lucentis® and Avastin® are used in the treatment of diabetic retinopathy. These medicines are injected into the eye. They act as chemical sponges to “sop up” and bind to the “bad” chemical signals that are released by the retina as result of diabetic damage. These medicines can be used to treat macular edema (swelling) and neovascularization (abnormal blood vessel growth).
4) Vitrectomy: The abnormal retinal blood vessels that develop as a result of diabetic retinopathy can bleed into the vitreous cavity of the eye. This can result in new floaters or significant sudden visual loss. In addition, to causing visual loss the blood can interfere with laser treatment of the retina. As a result, a surgery called a vitrectomy is required. A vitrectomy allows for removal of the blood from the eye and permits the surgeon to perform laser directly inside of your eye. Vitrectomy is also necessary to treat any significant traction on the retina produced by abnormal blood vessels. Your retinal surgeon will discuss this surgical procedure with you further if it is required.
-
What happens during laser treatment?
Before the laser, we will dilate your pupil and apply drops to freeze the front of the eye. The area behind your eye also may be frozen to prevent discomfort. The lights in the office will be dim. As you sit facing the laser machine, we will hold a special lens to your eye to prevent the lid from closing. During the procedure, you may see flashes of light. These flashes eventually may create a stinging sensation that can be uncomfortable. You will need someone to drive you home after laser. Because your pupil will remain dilated for a few hours, you should bring a pair of sunglasses. For the rest of the day, your vision will probably be a little blurry. If your eye has increasing pain or you develop nausea or vomiting, you should call our office.
-
What happens during the eye injections?
Anesthetic drops will be applied to freeze the surface of your eye. A speculum (spring) will be used to hold your eye open. An iodine solution will then be placed on the surface of the eye to sterilize it. You will be asked to look up or behind you to correctly rotate your eye. The medicine will then be injected by your specialist. It is normal to feel a sharp pinch, pressure or popping sensation at the time of the injection. Any discomfort is usually temporary. The remaining iodine solution will then be flushed from your eye. It is normal for the eye to be red after the procedure. New temporary floaters are also common.
-
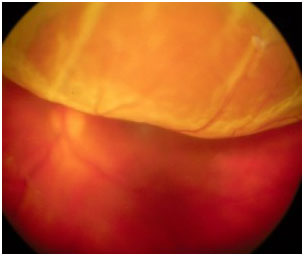
Epiretinal Membrane
An epiretinal membrane or wrinkle is a thin sheet of cells and/or vitreous jelly that is stuck on the retina. If vision is affected then surgery can be performed to remove the wrinkle and improve the vision in most cases. The risk of surgery includes cataract formation and retinal detachment. If surgery is performed it can take 6 months to 1 year for vision to improve.
An epiretinal membrane (also known as a macular pucker or cellophane maculopathy) is a condensation of a fibrous “membrane” on the surface of the retina. Often it is a result of the vitreous (Jelly that fills the eye) contracting and pulling off from the back surface of the eye. When it does so, it can leave a sheet of vitreous behind, like the skin of an onion stuck on the retina. Different types of cells can then multiply and cause further contraction of this sheet of vitreous on the surface of the retina. The “macula” is the center of the retina where the highest visual acuity is obtained. This is the part of the retina that is crucial for reading and detailed central vision. Membranes can cause the surface of the macula to become wrinkled and more opaque, like a layer of plastic wrap over a camera film. This can cause distortion or blurring of central vision.
ERMs can be associated with a variety of eye conditions, retinal tears, retinal detachments, eye inflammation, and vitreous hemorrhage. However, large proportions ERMs occur without any previous eye problems.
Visual acuity decreases to a level depending on how distorted the macular surface becomes. Some patients will have minimal vision distortion; others may have severe loss to the level of legal blindness. Sometimes even though your vision reading the eye chart may be quite good, the vision will still functionally be very poor due to distortion (straight lines appear bent, wrinkled).
The decision on trying to repair the membrane depends on how impaired vision has become. This is often determined by whether or not you can read with that eye alone (ie. Cover your good eye). If untreated the epiretinal membrane may remain stable or may continue to increase its distortion and cause further vision loss in the eye.
-
What can be done for an epiretinal membrane?
When vision is significantly impaired a surgical procedure called an vitrectomy and membrane peel can be performed. This procedure involves the removal of the vitreous gel from the eye. The epiretinal membrane is then gently grasped and peeled from the surface of the macula. Once the membrane is removed the traction on the retina is relieved and the macula can begin to flatten and become smoother. The vitreous gel is replaced with a special saline fluid during surgery and gradually your body replaces it with naturally produced fluid. Sometimes your retinal surgeon will decide to replace the vitreous with an air or gas bubble to help flatten the retina. The air bubble gradually goes away on its own and is replaced by the eyes normal intraocular fluid. Three small self-sealing incisions are made into the eye to perform the surgery. Occasionally, dissolving sutures are used.
-
What can I expect after surgery?
There is usually very little pain. It is common for patients to experience mild irritation for a few days after surgery. The use of an eye patch is recommended for 3 days. You will be given an eye shield which should be worn while sleeping for approximately 1 week. You will be given a prescription for eye drops to be used for 2–4 weeks. Severe pain or nausea and vomiting are indications to call your surgeon immediately. The eyelids are usually swollen for the first couple of weeks, but this gradually resolves thereafter. Vision is often very blurry for the first few days. An improvement in vision usually takes a few months to be noticed. Vision will usually slowly continue to improve in the months following surgery and can take up to 2 years to be maximally improved.
-
What are the risks of the procedure?
There are always risks associated with surgical procedures. A retinal detachment occurs in about 1-3% of patients but is usually treatable with further surgery. The intraocular pressure is transiently elevated in about 20% of patients. This is usually well controlled with eye drops and temporary. However, the inconvenience of additional office visits or medical therapies may be necessary.
The most severe complications occur less frequently: the risk of severe hemorrhage, infection, irreparable retinal detachment or complications from anesthesia occurs in approximately one in several thousand cases. These complications could result in irreversible blindness. Rarely double vision or eyelid droop may develop and need to be repaired with further surgery.
The most common side effect of epiretinal membrane surgery is cataract development. Cataract is a side effect of vitrectomy surgery, regardless of the underlying diagnosis. It often begins to develop by 6 to 12 months after surgery; however, it can develop sooner. If necessary, it can be surgically removed in the future, and an intraocular lens can be implanted.
The risks of the procedure are far outweighed by the benefits to your vision by removing the membrane. Usually we expect a significant improvement in both visual acuity and central distortion.
-
What follow-up is necessary?For the benefit of the patient, it is important to monitor the status of the eye following surgery. We usually see the patient one day, 1-2 weeks, 6-8 weeks, and then 3 or 4 months after surgery. These may be modified by your doctor. We will give you written directions after surgery about the care of your eye and follow up appointments. After surgery you should expect your eye to be red. If there is increasing pain or a perceived significant decrease in vision or other concerns you should call our office Anju Eye Care.
Laser Treatment
Summary:Laser is a high energy beam of light that can be used to cut or burn to treat eye disease. Burning laser can be used to treat leakage, new blood vessels or retinal tears. Cutting laser can be used to treat secondary cataracts or to perform refractive surgery. Laser treatments take only a few minutes. No special care is needed after most laser treatments. A special type of laser called photodynamic therapy (PDT) does require special care. An individual receiving PDT cannot be exposed to sunlight or intense lights for at least 48 hours or they are risk of developing a skin burn.
-
What is Laser Treatment?
The word LASER stands for “Light Amplification by Stimulated Emission of Radiation”. Laser is a high energy beam of light that can cut or burn tissue. There are many different types of lasers used to treat eye disease.
The general intent of laser surgery to the retina is to preserve your existing vision. The goal is to stop the progress of your eye disease. Do not expect it to improve your vision unless the doctor tells you it will.
At the doctor’s office you will have eye drops to enlarge your pupil and numb the front surface of your eye. Some laser procedures require an injection of freezing to numb the entire eye. You will sit at the laser in a dimly lit room, with your head supported by a chin and forehead rest. The doctor will place a special contact lens on your eye to focus the laser beam accurately. There is no incision or cutting into the eye. The doctor directs the laser light through the dilated pupil to the retina. Try to remain calm and do not move or squeeze your eyelids. When the doctor “fires” the laser, you may see a flash of light and feel a sensation of ache that can feel a bit uncomfortable. Sometimes the ache will feel like it is radiating backwards from your eye. The laser treatment usually takes from 5 to 15 minutes. No special eye care is required afterward. An eye patch is not necessary unless you had an injection of local anesthetic.
Your vision will be blurry for about 5-30 minutes following the laser. You do not have to remain at the office after your treatment. Arrange to have someone available to take you home. You may wish to wear dark glasses as your eyes will be sensitive to light while the pupil is large. You may take Tylenol if you experience any aching or irritation.
The doctor will need to see you again at some point following the laser to check your eye. More than one laser treatment is necessary in many cases to achieve the intended goal.
Laser treatment has been proven to be an effective method of reducing the risk of severe vision loss. Some types of peripheral laser treatment can cause swelling of the retina. This often results in blurring of vision which is usually temporary. Extensive treatment, necessary to treat certain eye diseases, can cause some peripheral vision loss and reduction in “night vision”, however most people do not notice this. Your doctor will discuss this with you if it is a possibility with your type of laser treatment. Every effort is made to keep visual loss at a minimum while controlling the disease process that is threatening your eyesight.
If you are receiving laser to repair a retinal tear, it is important to know that the laser will not remove floaters or haziness. The laser is used to seal the retinal tear, but is not able to remove blood, pigment or other debris floating in your eye. Time, usually a month or two will help to reduce the number and severity of floaters in your vision.
Ophthalmic laser surgery is a safe, precise and effective method of treating many retinal diseases. Your doctor will discuss your individual eye condition, treatment plan and expected outcome with you.
-
What is a “Macular Hole”?
The “macula” is the center of the retina where the highest visual acuity is obtained. A macular hole is a full thickness defect in this important location of the retina. This is like a hole in the center of the film in your camera. This hole is the result of traction of the vitreous on the retina. The vitreous is a jelly-like substance which fills the central cavity of the eye. In some the vitreous is firmly attached to the macula. As the vitreous “shrinks” and “collapses” with age it can pull on the center of the macula. This oblique traction can open a full thickness defect in the center of the macula (fovea). There is no actual loss of tissue in the hole. Visual acuity decreases markedly to a level depending on the size of the hole, but usually to the level of legal blindness. Visual loss is due to disruption of the normal physiologic arrangement of the photoreceptors (light sensing cells) in the center of the macula, and due to collection of fluid under the retina in this area.
Macular holes develop because of traction on the central retina by the vitreous. Surgical treatment to remove the vitreous from the eye followed by injection of a gas bubble is successful in repairing the hole 90-95% the time. Without surgery, a macular hole will not improve.
-
What can be done for a macular hole?
Up until about 1992, there was nothing that could be done to alter the status of a macular hole. We now perform a surgical procedure that involves removing the vitreous gel and internal limiting membrane (the innermost layer of the retina) from the eye to relieve any traction and distortion of the macula. When the traction is relieved the macula can “relax” back into its normal anatomical position which closes the macular hole.
The vitreous gel is replaced with a mixture of air and a slowly dissolving inert gas (C3F8 or SF6) at the end of your surgery. The surface tension of the gas bubble acts to aid in closure of the macular hole. In order to maximize the effect of the bubble, you may be requested to maintain face down (prone) positioning or positioning on your side positioning for a period of time after your surgery. This ensures that the gas bubble will stay in contact against the macular hole. Your surgeon will discuss your positioning instructions with you.
-
What can I expect after surgery?
Gas placed within the eye will be gradually reabsorbed by the eye during a 2-8 week period following surgery. As the bubble is reabsorbed, the vitreous cavity refills with a fluid that is naturally produced by the eye. Vision will be markedly reduced immediately after surgery since you cannot see well through the bubble. As the bubble reabsorbs you will gradually see more and more. You should not, however, expect to experience significant improvement in vision until at least 6 weeks after surgery, and final visual acuity outcome may not be obtained for up to 2 years following the macular hole repair. You may not fly in an airplane or travel to high elevations (i.e. mountains) until the bubble is almost completely gone. Some types general anesthetic agents must be avoided (nitrous oxide or laughing gas) while there is a gas bubble in your eye.
There is usually very little pain. It is common for patients to experience mild irritation for a few days after surgery. The use of an eye patch is recommended for 3 days. You will be given an eye shield which should be worn while sleeping for approximately 1 week. You will be given a prescription for eye drops to be used for 2–4 weeks. Severe pain or nausea and vomiting are indications to call your surgeon immediately, even if it is the evening or weekend. It may be an indication that the pressure in the eye is too high. The eyelids are usually swollen for the first couple of weeks, but this gradually resolves thereafter. As the gas bubble shrinks in your eye, you will begin to notice a fluid level when looking through the operated eye. This level will gradually change with time. Often, satellite bubbles will form, giving the appearance of fish eggs or small balloons when you look through the operated eye. This is normal and is no cause for alarm.
-
What are the risks of the procedure?
There are always risks associated with surgical procedures. A retinal detachment occurs in about 1-3% of patients but is usually treatable with further surgery, often with little or no adverse effect on your final vision. The intraocular pressure is transiently elevated in about 20% of patients. Often a feeling of nausea or eye pain will accompany elevated intraocular pressure. This is usually well controlled with eye drops and temporary. However, the inconvenience of additional office visits or medical therapies may be necessary.
The most severe complications occur less frequently: the risk of severe hemorrhage, infection, irreparable retinal detachment or complications from anesthesia occurs in approximately one in several thousand cases. These complications could result in irreversible blindness. Rarely double vision or eyelid droop may develop and need to be repaired with further surgery.
The most common side effect of macular hole surgery is cataract development. A cataract is a side effect of vitrectomy surgery, regardless of the underlying diagnosis. It begins to develop in almost all patients by 6 to 12 months after surgery; however, it may develop sooner. If necessary, it can be surgically removed in the future, and an intraocular lens can be implanted.
The risks of the procedure are far outweighed by the benefits to your vision by repairing the macular hole. Up to 15% of patients may develop a macular hole in their other eye, or suffer vision loss in their other eye from some other cause Therefore, repair of the macular hole is very important.
-
What follow-up is necessary?
For the benefit of the patient, it is important to monitor the status of the eye following surgery. We usually see the patient one day, 1-2 weeks, 6-8 weeks, and then 3 or 4 months after surgery. These may be modified by your doctor. We will give you written directions after surgery about the care of your eye and follow up appointments. After surgery you should expect your eye to be red. If there is increasing pain or a perceived significant decrease in vision or other concerns you should call our office at Anju Eye Care.
-
Plaquenil Toxicity

There are several medications that are helpful in managing the problems associated with diseases such as lupus erythematosus, rheumatoid arthritis, and other inflammatory and dermatologic conditions. Unfortunately, despite their many benefits, both medications, chloroquine (Aralen) or its analogue, hydroxychloroquine (Plaquenil), carry with them a very small risk of permanent vision loss.
Eye screening by an ophthalmologist is important to help identify any damage to the eye at the earliest stage possible. This is very important as once damage has occurred it cannot be reversed. In addition, should damage occur, it can continue to worsen even if (hydroxy)chloroquine is stopped. Despite these risks, your referring doctor believes that at this time the benefits to you in taking these medications are greater than the risks to your eyes.
Now that you have been referred to the ophthalmologist for eye screening, you will be assessed on an annual basis for as long as you are taking chloroquine or hydroxychloroquine. Even if you do stop the medication, it may be necessary to continue eye screening for up to 5 years after you have stopped.
There are several ways to test for damage from chloroqine and hydroxychloroquine to the eye. In Anju Eye Care Hospital, we perform many of these tests on an annual basis to maximize our chances at picking up any early changes from (hydroxy)chloroquine. As part of the Anju Eye Care (hydroxy)chloroquine screening protocol you will undergo tests once per year at the hospital and once per month at home.
The following tests are used as part of the Anju Eye Care (Hydroxy)chloroquine Screening Protocol:
- Amsler grid: This small grid is given to you to test once per month at home. It should be held at approximately 12 inches (30 cm) from the face. If you wear glasses for reading, you should use them for the test. Closing one eye, look directly at the centre dot, then without moving your eye assess the rest of the grid for faded or missing areas, or loss of central vision. Once one eye has been tested, repeat the process for the other eye. If you find a problem with your vision, you should contact your ophthalmologist for an in-person examination.
- Color photography of the retina and cornea: This test is to look to see if there has been any accumulation of medication in the cornea, or damage to the retina while maintaining a permanent record for comparison the following year.
- Visual field (10-2): This test is to identify whether or not there is any loss of central field of vision. This test is performed at the hospital, takes less than 10 minutes per eye, and requires you to look at small flashing lights.
- D-15 colour testing: This test requires you to line up a number of coloured circles in order. Damage from (hydroxy)chloroquine can cause loss of colour vision.
- Multifocal ERG: This test is a relatively new test, which at times can identify changes from (hydroxy)chloroquine at a stage earlier than any of the other tests. Unfortunately other problems with vision can lead to abnormal results. For this reason, although we do use this test, it is often repeated prior to making any recommendations regarding changing or stopping (hydroxyl)chloroquine.
- Fluorescein angiography: If damage from (hydroxy)chloroquine is suspected, an ophthalmologist may order this test to help confirm the diagnosis. This test involves injecting dye into the arm followed by photographs of the back of the eye. (Hydroxy)chloroquine damage can show up as a ring of damage around the central part of vision. If any problems are identified with testing at the hospital, you will be contacted directly by the ophthalmologist or a member of the eye care team.
If you notice a problem when self-testing, you should contact your ophthalmologist directly.
As the testing centre at the Anju Eye Care hospital has limited spots available it is very important that you attend your testing appointment. If you cannot make your appointment please let the testing centre or your ophthalmologist’s office know as early as possible so that your testing appointment can be given to someone else.
-
What is a retinal detachment?
The inside of the eye is filled with a gel like substance called the vitreous. The vitreous has a jello or egg-white consistency when we are young, and is firmly attached to the front of the eye on the inside (called the vitreous base). The retina is the very thin tissue that lines the inside of the eye cavity like wallpaper. When we look at something, the retina acts like the film in a camera and captures the image. The retina is attached to the wall of the eye only at the very front and at the back of the eye where the optic nerve goes to the brain. The vitreous is more lightly attached to the rest of the retina. Over time, the vitreous gradually becomes thinner and more liquified. It eventually collapses inwards, and separates from the retina. This separation of the vitreous from the retina is called a posterior vitreous detachment (PVD). PVD’s are typically harmless and cause increased floaters in the eye. In some cases, the traction on the retina may create a tear. Retinal tears frequently lead to retinal detachment as fluid from the vitreous seeps underneath the retina. This fluid causes the retina to separate and detach from the outer layers of the eye. Retinal detachment can also develop from holes in the peripheral retina which develop in areas of retinal thinning.
Retinal detachment is a serious problem and can result in permanent visual loss. It is a medical emergency and anyone experiencing symptoms of retinal detachment should seek assessment from an eye care professional immediately.
Retinal detachments develop as a result of traction on the retina by the vitreous that first creates a retinal hole, then with continued traction leads to a retinal detachment. Treatment includes removing the vitreous from the eye with a gas bubble and laser or placing a silicone band around the eye, with a gas bubble and a freezing probe. Given enough time, all vision will be lost without surgery. Surgery is successful in approximately 85% of cases, with repeat surgery leading to re-attachment of the retina in 95% of cases.
-
What are symptoms of retinal detachment?
The initial symptoms of retinal detachment may be quite mild. A sudden onset of flashing lights and multiple new floaters (little “cobwebs” or specks that float about in your field of vision) may occur. Flashes and floaters are often the symptoms of a retinal tear. After a retinal tear has occurred the retina may begin to detach. As the retina starts to detach changes in peripheral vision (outside vision) in one eye begin to occur. Loss of peripheral vision from the side top or bottom may advance towards the center of vision like a curtain, often in a “half moon” shape. This can progress to total vision loss. Sometimes, the symptoms of retinal detachment may go unnoticed until central vision is affected. Occasionally, a peripheral retinal detachment may be present without producing any symptoms at all. This is one reason regular eye exams with your ophthalmologist are very important.
-
Who is at risk for retinal detachment?
A retinal detachment can occur at any age, but it is more common in people over age 40. You should discuss your risk for retinal detachment with your ophthalmologist. Risk factors for retinal detachment include:
- Myopia (nearsightedness)
- Previous retinal detachment in the other eye
- Family history of retinal detachment
- Cataract surgery
- Eye trauma
- Other predisposing eye diseases or disorders
- Predisposing genetic conditions
-
How are retinal detachments repaired?
Retinal detachment can only be repaired with a surgical procedure. Your retinal specialist will discuss your surgery with you. There are three main types of surgical procedures for retinal detachment repair.
1. Pneumatic retinopexy: This procedure is used to treat retinal detachments with very specific characteristics. A temporary gas bubble is injected into the vitreous cavity of the affected eye. The surface tension of the gas bubble acts to seal off the retinal tear or hole. Your eye can then pump out the fluid that has accumulated under the retina. The success of this procedure requires strict positioning of your head after the gas injection to ensure that the bubble seals off the retinal break. The retinal tear is directly treated with cryopexy (a super cooled probe applied to the outside of the eye) or retinal laser to prevent the detachment from returning once the bubble is absorbed by your eye.
2. Scleral buckle: This is the type of procedure most commonly used for people who have a retinal detachment but have not had cataract surgery yet. All retinal tears are directly treated with cryopexy (a super cooled probe applied to the outside of the eye). A silicone band is then placed around the outside of the eye behind the insertion of the 4 major muscles that move the eye. This indents the eye wall to move it closer to the retina. This acts to release the pulling of the vitreous gel on the retina to allow closure of retinal breaks. Fluid is then removed from the front of the eye to decrease pressure inside the eye. Finally, a temporary gas bubble is injected into the eye. The surface tension of the gas bubble acts to seal off the retinal tear or hole. Following the surgery your retinal specialist may ask you to position your head in a specific way.
3. Pars plana vitrectomy: This is the type of procedure most commonly used for people who have a retinal detachment and have had prior cataract surgery. Three small incisions are made through the sclera (the white of the eye). Your surgeon then uses a microscope and a special lens system to operate directly within your eye. A special instrument, called a vitrector, is used to remove as much vitreous gel as possible. This eliminates any traction on the retina. The fluid under the detached retina and within the vitreous cavity is then drained. A probe is then inserted into the eye so that laser can be used to permanently seal off any retinal breaks. A slow absorbing gas is then injected into the eye to completely fill up the vitreous cavity. The surface tension of the gas acts to seal of the retinal breaks while the laser spots are maturing. Your surgeon may request that you position your head in a specific way after the surgery to position the gas bubble onto the retinal breaks and detached retina. The gas bubble will be slowly absorbed by your eye at different rates depending on the type of gas used. Sometimes silicone oil is placed within the vitreous cavity instead of gas. If this is the case, a second surgery is usually required to remove the oil. Sometimes, a combination of both scleral buckle and vitrectomy surgeries will be performed. Your retinal specialist will discuss which surgery will be best for you.
-
What is intraocular gas and silicone oil?
Gas placed within the eye will be gradually reabsorbed by the eye during a 2-8 week period following surgery. As the bubble is reabsorbed, the vitreous cavity refills with a fluid that is naturally produced by the eye. Vision will be markedly reduced immediately after surgery since you cannot see well through the bubble. As the bubble reabsorbs you will gradually see more and more. You should not, however, expect to experience significant improvement in vision until at least 6 weeks after surgery, and final visual acuity outcome may not be obtained for up to 2 years following the retinal detachment repair. You may not fly in an airplane or travel to high elevations (i.e. mountains) until the bubble is almost completely gone. Some types general anesthetic agents must be avoided (nitrous oxide or laughing gas) while there is a gas bubble in your eye.
Silicone oil does not reabsorb on its own, instead it must be removed with an additional surgical procedure from 2 months to 2 or more years after the original surgery. If silicone oil is utilized, there is no risk from flying or from having a general anesthetic.
Over 90% of retinal detachments can be successfully treated. However often more than one procedure is necessary. Unfortunately, even after multiple attempts at retinal detachment repair, treatment sometimes fails and vision may be lost permanently. Visual outcome is not always predictable. Visual results are usually best if the retinal detachment is repaired before the macula (the center region of the retina responsible for fine, detailed vision) detaches. This is why urgent surgery is often required. The final visual result may not be known for up to several months following surgery.
-
What can I expect after surgery?The eye may be quite sore for approximately 1 to 2 weeks following sclera buckling surgery. There is usually very little pain following pneumatic retinopexy and vitrectomy procedures. However, it is common for patients to experience mild irritation for a few days after surgery. The use of an eye patch is recommended for 3 days, or until the eye stops tearing. You will be given an eye shield which should be worn while sleeping for approximately 1 week. You will be given a prescription for eye drops to be used for 2–4 weeks. Severe pain or nausea and vomiting are indications to call your surgeon immediately even if it is the evening or weekend. The eyelids are usually swollen for the first couple of weeks, but this gradually resolves thereafter. As the gas bubble shrinks in your eye, you will begin to notice a fluid level when looking through the operated eye. Some vision should be present above the fluid level. The top field of vision should gradually enlarge as the bubble shrinks. Often, satellite bubbles will form, giving the appearance of fish eggs or small balloons when you look through the operated eye. This is normal and is no cause for alarm. If your vision is good one day, then much worse the next, you may have developed a recurrent retinal detachment. You should contact our office immediately, even if it is the evening or weekend.
-
What follow-up is necessary?
For the benefit of the patient, it is important to monitor the status of the eye following surgery. We usually see the patient one day, 1-2 weeks, 6-8 weeks, and then 3 or 4 months after surgery. These may be modified by your doctor. We will give you written directions after surgery about the care of your eye and follow up appointments. After surgery you should expect your eye to be red. If there is increasing pain or a perceived significant decrease in vision or other concerns you should call our office at Anju Eye Care Hospital.
-
What are floaters and flashes and why are they important?
To help understand this question it is important to first understand the anatomy of the eye. The inside of the eye is filled with a gel like substance called the vitreous. The vitreous has a jello or egg-white consistency when we are young, and is firmly attached to the front of the eye on the inside (called the vitreous base). The retina is the very thin tissue that lines the inside of the eye cavity like wallpaper. When we look at something, the retina acts like the film in a camera and captures the image. The retina is attached to the wall of the eye only at the very front and at the back of the eye where the optic nerve goes to the brain. The vitreous is more lightly attached to the rest of the retina. Over time, the vitreous gradually becomes thinner and more liquid. It eventually collapses (analogy like a collapsed spider web), and separates from the retina. This separation of the vitreous from the retina is called a posterior vitreous detachment (PVD). PVD’s are typically harmless and cause increased floaters in the eye. In some cases however the traction on the retina may create a tear. Retinal tears frequently lead to retinal detachments as fluids seeps underneath the retina, causing it to separate and detach from the outer layers of the eye.
-
Are all floaters a sign of a problem?
No. Many people experience floaters when they are young and without having a PVD. These floaters are just condensations of the protein gel in the eye. They float in the cavity of the eye and cast tiny shadows on the retina. Floaters are more likely to develop as we age and are more common in people who are very nearsighted, have diabetes, or who have had a cataract operation. There are other, more serious causes of floaters, including infection, inflammation (uveitis), hemorrhaging, retinal tears, and injury to the eye. In most cases, floaters are part of the natural aging process and simply an annoyance. They can be distracting at first, but eventually tend to “settle” at the bottom of the eye, becoming less bothersome. They usually settle below the line of sight and do not go away completely. Most people have floaters and learn to ignore them; they are usually not noticed until they become numerous or more prominent. Floaters can become apparent when looking at something bright, such as white paper or a blue sky.
For people who have floaters that are simply annoying, no treatment is recommended. Floaters can rarely be so dense and numerous that they significantly affect vision. Usually with time these will settle down and be acceptable. In very rare cases , a vitrectomy may be needed. A vitrectomy removes the vitreous gel, along with its floating debris, from the eye. The vitreous is replaced with a salt solution. Because the vitreous is mostly water, you will not notice any change between the salt solution and the original vitreous. Surgery is not recommended unless the floaters seriously interfere with vision.
-
How do you treat a retinal tear?
If you develop a retinal tear it should be treated with laser to create a scar adhesion between the retina and the outer layers of the eye. Laser uses light to create heat at the spot where it is focused. This heat burns the tissue which heals as a scar adhering the tissues together. The retinal function in the areas of the laser is lost because the tissue is destroyed. Realize however that the area of the retinal tear is already not functioning as a result of the tear and that the tiny blind spot caused by the laser is only minimally larger. The laser treatment helps to prevent a subsequent retinal detachment in the vast majority of cases.
-
What do I watch out for after laser treatment of my retinal tear?
Any sudden increase in new floaters again could signify another tear and should be assessed. Also any loss of peripheral vision (like a shade or curtain being drawn from your peripheral vision toward the central vision) may be a sign of retinal detachment and needs to be assessed promptly.
-
What Is Retinopathy Of Prematurity (ROP)?
Retinopathy of prematurity (historically called Retrolental Fibroplasia) is a potentially blinding eye disorder that primarily affects premature infants weighing about 2¾ pounds (1250 grams) or less that are born before 31 weeks of gestation (A full-term pregnancy has a gestation of 38–42 weeks). The smaller a baby is at birth, the more likely that baby is to develop ROP. This disorder—which usually develops in both eyes—is one of the most common causes of visual loss in childhood and can lead to lifelong vision impairment and blindness. ROP was first diagnosed in 1942.
-
How many infants have ROP?
Today, with advances in neonatal care, smaller and more premature infants are being saved. These infants are at a much higher risk for ROP. The disease improves and leaves no permanent damage in milder cases of ROP. About 90 percent of all infants with ROP are in the milder category and do not need treatment. However, infants with more severe disease can develop impaired vision or even blindness.
-
What causes ROP?
ROP occurs when abnormal blood vessels grow and spread throughout the retina, the tissue that lines the back of the eye. These abnormal blood vessels are fragile and can leak, scarring the retina and pulling it out of position. This causes a retinal detachment. Retinal detachment is the main cause of visual impairment and blindness in ROP.
Several complex factors may be responsible for the development of ROP. The eye starts to develop at about 16 weeks of pregnancy, when the blood vessels of the retina begin to form at the optic nerve in the back of the eye. The blood vessels grow gradually toward the edges of the developing retina, supplying oxygen and nutrients. During the last 12 weeks of a pregnancy, the eye develops rapidly. When a baby is born full-term, the retinal blood vessel growth is mostly complete (The retina usually finishes growing a few weeks to a month after birth). But if a baby is born prematurely, before these blood vessels have reached the edges of the retina, normal vessel growth may stop. The edges of the retina—the periphery—may not get enough oxygen and nutrients.
Scientists believe that the periphery of the retina then sends out signals to other areas of the retina for nourishment. As a result, new abnormal vessels begin to grow. These new blood vessels are fragile and weak and can bleed, leading to retinal scarring. When these scars shrink, they pull on the retina, causing it to detach from the back of the eye.
-
Does oxygen administered to babies cause ROP?It was thought at one time that too much oxygen caused ROP. However, many very premature babies would not survive or would be mentally impaired without oxygen. Now there are many advances in neonatal medicine which help immature lungs develop and work better, so less oxygen can be used for the premature babies. It is also thought that not enough oxygen could cause ROP. Supplemental oxygen as required has been shown to not worsen active prethreshold ROP. Oxygen should be used as directed by your neonatologist.
-
Do neonatal intensive care unit (NICU) lights worsen ROP?Studies have shown no correlation between light exposure and the development of ROP.
-
Are there different stages of ROP?
ROP is classified in five stages, ranging from mild (stage I) to severe (stage V):
Stage I — Mildly abnormal blood vessel growth. Many children who develop stage I improve with no treatment and eventually develop normal vision. The disease resolves on its own without further progression.
Stage II — Moderately abnormal blood vessel growth. Many children who develop stage II improve with no treatment and eventually develop normal vision. The disease resolves on its own without further progression.
Stage III — Severely abnormal blood vessel growth. The abnormal blood vessels grow toward the center of the eye instead of following their normal growth pattern along the surface of the retina. Some infants who develop stage III improve with no treatment and eventually develop normal vision. However, when infants have a certain degree of Stage III and “plus disease” develops, treatment is considered. “Plus disease” means that the blood vessels of the retina have become enlarged and twisted, indicating a worsening of the disease. Treatment at this point has a good chance of preventing retinal detachment.
Stage IV — Partially detached retina. Traction from the scar produced by bleeding, abnormal vessels pulls the retina away from the wall of the eye.
Stage V — Completely detached retina and the end stage of the disease. If the eye is left alone at this stage, the baby can have severe visual impairment and even blindness. Most babies who develop ROP have stages I or II. However, in a small number of babies, ROP worsens, sometimes very rapidly. Untreated ROP threatens to destroy vision.
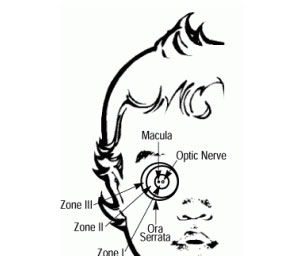
We also refer to zones of involvement in the retina, as pictured in the graphic of the retina:
Zone One is centered on the Macula (which is the area of central vision needed for reading).
Zone Two refers to an area that is doughnut shaped that extends to the edge closest to the nose.
Zone Three refers to the crescent shaped area toward the ear.
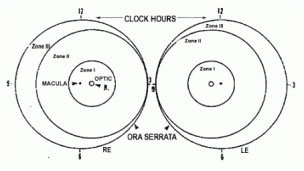
If disease appears in Zone One (as can happen with extremely low birthweight infants) damage to the retina tends to be more severe. IF Zone Three is affected, the premature infant will tend to have mild involvement, leading to useful vision.
-
How is ROP treated?
The most effective proven treatments for ROP is laser therapy. Laser therapy “burns away” the periphery of the retina, which has no normal blood vessels. Laser treatment destroys the peripheral areas of the retina, slowing or reversing the abnormal growth of blood vessels. Unfortunately, the treatments also destroy some side vision. This is done to save the most important part of our sight—the sharp, central vision we need for “straight ahead” activities such as reading, sewing, and driving.
Laser treatment is performed only on infants with advanced ROP, particularly stage III with “plus disease.” New evidence is pointing to benefit for earlier laser treatment.
In the later stages of ROP, other treatment options include:
Scleral buckle: This involves placing a silicone band around the eye and tightening it. This keeps the vitreous gel from pulling on the scar tissue and allows the retina to flatten back down onto the wall of the eye. Infants who have had a sclera buckle need to have the band removed months or years later, since the eye continues to grow; otherwise they will become nearsighted. Sclera buckles are usually performed on infants with stage IV or V.
-
What is Vitrectomy?
involves removing the vitreous and replacing it with a saline solution. After the vitreous has been removed, the scar tissue on the retina can be peeled back or cut away, allowing the retina to relax and lay back down against the eye wall. Vitrectomy is performed at stage V and in some cases in stage IV.
-
What happens if treatment does not work?
While ROP treatment decreases the chances for vision loss, it does not always prevent it. Not all babies respond to ROP treatment, and the disease may get worse. If treatment for ROP does not work, a retinal detachment may develop. Often, only part of the retina detaches (stage IV). When this happens, no further treatments may be needed, since a partial detachment may remain the same or go away without treatment. However, in some instances, physicians may recommend treatment to try to prevent further advancement of the retinal detachment (stage V). If the center of the retina detaches, central vision is threatened, and surgery may be recommended to try and reattach the retina. Despite best efforts in rare cases blindness may still result.
-
Are there other risk factors for ROP?
In addition to low birth weight and how early a baby is born, other factors contributing to the risk of ROP include anemia, blood transfusions, respiratory distress, breathing difficulties, and the overall health of the infant.
-
Can ROP cause other complications?
Yes. Infants with ROP are considered to be at higher risk for developing certain eye problems later in life, such as retinal detachment, myopia (nearsightedness), strabismus (crossed eyes), amblyopia (lazy eye), and glaucoma. In many cases, these eye problems can be treated or controlled.
-
What is Vein Occlusions?
A branch retinal vein occlusion (BRVO) is a blockage of one of the blood vessels in the retina. Risk factors include arteriosclerosis, high blood pressure and diabetes, although many people who develop BRVOs do not have any of these risks. BRVOs can lead to leakage of the retina that can reduce vision, and to new blood vessels that can break and bleed. Treatment includes injections of medication into the eye and laser treatment.
-
What Is A Branch Retinal Vein Occlusion?
A branch retinal vein occlusion (BRVO) is a blockage of one of the small blood vessels that drains blood from the retina. The retina is the light-sensitive nerve tissue lining the back of the eye.
Like film in a camera, the retina continually “takes pictures” of everything you look at. When part of the retinal vein becomes blocked, the retinal blood flow slows or stops. Suddenly and usually without warning, a patch of retina loses some of its “picture-taking” function and you may be aware that part of your field of vision has darkened.
-
Why Is Vision Lost?
Normally, the retina is nourished by oxygen-rich blood that is brought to it by arteries and drained away by veins. When a vein – a drainage channel – is blocked, blood backs up, leading to bleeding and swelling (edema) in the retina which hampers its nourishment.
The extent of damage and the visual symptoms produced depend on the size of the blocked vein and its exact location. If the blockage occurs toward the peripheral part of the retina, you may hardly notice it. But if it occurs in or near the macula – the central zone of the retina that is critical for sharp vision – and causes it to swell, vision is likely to be reduced or distorted.
A more serious threat to vision can develop later from a complication called neovascularization (neo = new, vascular = blood vessels). A month or more after the BRVO, new blood vessels may begin to appear in the retina, as if they were trying to renourish it. These are not normal blood vessels as they are very fragile and bleed easily. They are dangerous to the eye because they can lead to still other problems that damage vision.
Neovascularization only occurs in about one in five BRVO patients. If it develops in your eye, it should be treated before causing harm. In most cases there are no warning symptoms; but occasionally there are, such as the sudden appearance of new floaters (translucent specks that move about in your field of vision) or a sudden decrease in vision.
-
What Causes a Vein Occlusion?
Several factors combine to bring on an occlusion. The usual situation is that something causes the blood flow in a retinal vein to slow down so much that it permits a clot to form there. The clot prevents blood from flowing freely.
The most common reason for slowed venous blood flow is, surprisingly, a hardened artery (arteriosclerosis). If a stiff artery happens to lie across a vein and compresses it, it can slow the flow of blood in that vein in the same way that stepping on a hose can obstruct the flow of water. Because arteriosclerosis occurs so often in people who have hypertension (high blood pressure), and diabetes they are considered to be a risk factor for the development of BRVO.
Other conditions that can lead to a BRVO are venous inflammation (vasculitis), which can plug the vein , and some rare blood conditions that produce a greater-than-normal tendency for blood to clot. Even estrogen medication (as in oral contraceptives) can introduce a slight risk of blood clotting.
In many cases no risk factors are found and simply the way your individual blood vessels lay one atop the other puts you at risk as you age.
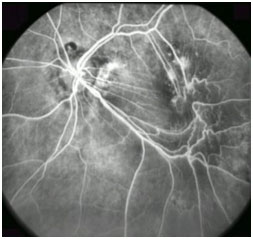
Retinal photographs may be taken to help determine the extent of the problem. An angiogram (photographs of blood vessels) may also be done. For this test, an orange-colored dye (fluorescein) is injected into a vein in your arm and is immediately followed by a series of retinal photographs that track the dye, and time its flow, as it travels through the eye’s blood vessels. The angiogram helps identify the exact site of the vein’s blockage, the extent of damage to capillaries (the smallest retinal blood vessels), the site of leakage and whether or not neovascularization has developed. OCT (optical coherence tomography) scans will be performed to monitor the position and extent of swelling within the retina.
Because BRVO can be associated with medical conditions that affect the rest of the body (high blood pressure, for example, which also increases the risk of a heart attack or stroke), you should be evaluated by our ocular stroke clinic. Our office will arrange this for you. (if not let us know so we can do so).
-
Treatment
Once a BRVO has occurred; there is no simple way to speed the healing process along. Eventually, over several months, the blocked vein may re-open on its own, or some nearby blood vessels (called collaterals) may develop and reroute the blood flow around the site of blockage. Either of these may help restore at least part of the lost retinal function.
If neovascularization develops, a type of laser surgery called panretinal photocoagulation (PRP) can help reduce or even eliminate the abnormal blood vessels. PRP is not intended to improve vision directly. It reduces the risk of further vision loss from internal bleeding or, possibly, from a retinal detachment.
After a BRVO, the central retina (macula) sometimes remains swollen for months, reducing vision significantly. You may be treated with eye injections of special medicines called Avastin and Lucentis to help resolve or reduce the swelling, often more than once. These medicines were initially developed to treat wet age related macular degeneration. However, they are also very effective in reducing macular swelling (edema) caused by BRVO. Laser treatments may also be used to minimize the macular swelling. Your doctor will discuss these treatments with you.
Regular follow-up examinations are important to protect your eyesight. Your eyes should be checked regularly for potential late complications, such as neovascularization or macular edema, and for the development of a second vascular occlusion in either eye.
-
Pre-exam Instructions:
- Your appointment is expected to last approximately 1-2 hours due to pupil dilation, vision screening and consultation.
- Dilation can last from 1-2 hours after your appointment, therefore we recommend that you bring a driver or have an alternate mode of transportation to get home. Please bring sunglasses for your comfort.
- Please bring any corrective eyeglasses with you.
- Please bring a list of current medications with you.
- If you are diabetic, please bring a snack and any medications along with you in case of increased waiting times.
- Insurance and third party form completion will be your own responsible.
- For all patients comfort, we suggest that you do not bring small children to your appointment unless necessary.
If you know what your potential diagnosis is, please feel free to print off the information sheet from our website.
Also please feel free to bring a list of questions to ask your doctor about your condition, to help you remember what you were going to ask. Please also bring a list of your current medications, so we can keep your file up to date in case of emergency. If you are diabetic, please bring a snack and eat prior to attending your appointment if you can as the wait can be from 1-3 hours depending on the day.